


By Frank Pellikaan & Ed Westerhout
Rising longevity, low fertility and declining disability have serious implications for public finances. Although alternative assumptions on longevity and disability may alleviate or increase the pressure on public finances, public finances will become unsustainable if policy reforms fail to occur.
The world is on the eve of huge demographic changes. Worldwide, fertility rates are, from a historical perspective, very low. Mortality rates continue to decline. These changes will have serious implications for government budgets. As pension and health care systems are often organized on a pay-as-you-go basis, they are vulnerable to structural demographic change. In many cases, in order to avoid losing control over government finances, these systems will therefore have to be reformed; this may imply an increase of contributions, a lowering of benefits, or a combination of both. Obviously, any of these reforms may affect the economy and the balance between generations.
This contribution assesses the relevance of these changes and their likely effects. It starts with a discussion of demographic and also epidemiological changes. Next, it describes the research we did on the likely fiscal and macroeconomic implications of these changes. Furthermore, we dig into the policy implications of our analysis.
Trends in demography and epidemiology
Worldwide, dramatic changes have occurred in fertility and mortality. The worldwide average total fertility rate has decreased, from a level of 4.9 children per woman in 1950-1955 to about 2.6 children per woman in 2005-2010.1 Details differ from country to country, but the trend of falling fertility applies to almost all countries. Fertility rates may remain low if they are part of a demographic transition towards lower mortality, lower fertility and higher educational attainment.2 For the future, many projection studies indeed assume that fertility rates will remain at their current low levels. UN (2009) even predicts a further decline of the total fertility rate towards 2.0 in 2045-2050.
The changes in mortality rates have been similarly large. Over the past few decades, mortality rates have been falling steadily in many countries in the world. As a result, life expectancy has increased strongly. In particular, worldwide average life expectancy at birth has increased from a level of 46.6 years in 1950-1955 to a level of 67.6 years in 2005-2010.3 Here, the variation across countries is large, but the trend of a strong increase in life expectancy is rather uniform. The single factor that is held responsible for a large part of the reduction in mortality is medical-technological progress.4 Progress in medical technology may continue in the future, allowing for further gains in life expectancy. Many projection studies indeed assume that mortality rates will fall and longevity will increase in the coming decades. UN (2009) predicts life expectancy at birth to achieve a level of 75.5 years in 2045-2050.
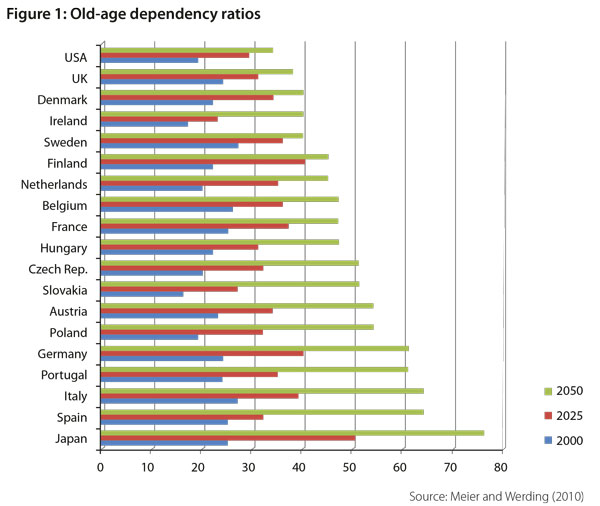
The result of low fertility rates and declining mortality rates is an increase in old-age dependency ratios.5 Figure 1 shows the expected development of old-age dependency ratios in a number of countries in the next four decades. What is striking is that the pattern of increasing old-age dependency ratios applies to all countries. Further, the changes ahead are huge. Indeed, in 2000-2050 the old-age dependency ratio is expected to increase by more than 50% in all countries and to more than double in the majority of the countries.
Old-age dependency ratios do not tell the whole story however, as disability rates have not been constant either. Disability rates among the elderly have been declining in many countries and, again, progress in medical technology seems to have played a role.6 Although obesity rates are increasing in many countries, it is quite likely that disability rates will keep falling further in the future.7
It should be stressed that prospects for the future are very uncertain, especially as the horizons involved are long. This is true both for demographic and epidemiological trends. In the case of demographics, projecting the future has often proven to be so difficult that one should be very cautious not to underestimate the range of possible future outcomes.8 Our numerical simulation study The trends described above raise questions about the sustainability of current public finances. Increasing life expectancy and declining disability ratios obviously affect public health care spending, both in acute health care such as hospitals and in long-term care such as nursing services for the elderly and the disabled. But they also affect labor market participation and the value of pension entitlements and thus have an impact on tax and social security revenues and public expenditures. Since public pension and health care systems are often financed on a pay-as-you-go basis, they cannot cope with rising longevity without being reformed.
How to measure the long-term sustainability of these systems? The threat of worsening fiscal sustainability will not show up immediately in deficit and debt ratios, but reveals itself only after a long period of time. Here, the concept of the sustainability gap is useful. The sustainability gap is a widely used measure to indicate the immediate and permanent change in the primary surplus ratio (in terms of GDP) that is required to restore financial sustainability. The sustainability gap thus captures the whole future of old-age dependency ratios and is therefore able to signal future problems with fiscal sustainability.
We have explored the impact of the trends described above on the sustainability gap in three scenarios, which we label as ‘living longer’, ‘living in better health’ and ‘living longer in better health’. Each of the scenarios represents a different set of assumptions on changes in life expectancy and disability ratios. The results presented are the differences between these scenarios and a base case scenario. For technical details on the calculations and the data that we have used we refer to our study.9 In that study, we have calculated the effects for various EU countries. Here, we will focus on the results for the EU average.
Results
The ‘living longer’ scenario
In the ‘living longer’ scenario we have assessed the impact that a further increase in life expectancy would have, compared to the base case scenario. This ‘living longer’ scenario corresponds to the idea that life expectancy may increase further in the future and especially that the mortality rates at older ages, i.e. those between 80 and 90, may decline at the same rate as those observed for younger people. This is in contrast with the argument underlying many projection studies that the gains in life expectancy may become much smaller in the future due to a biological limit to human life expectancy. However, it is in accordance with White (2002) who has found that over the last 40 years, the growth in life expectancy has not declined, but rather shows a slight acceleration. This suggests that if there is a biological limit to human life, life expectancy is not close to this limit at this moment or the limit evolves over time. Vaupel (1998) argues the same along a different line. If there is a biological limit, increases in life expectancy will be smaller for older people. However, historical reductions in mortality rates have been highest for people older than 80 years.
In accordance with this evidence, our ‘living longer’ scenario therefore assumes an increase of 8.2 years in life expectancy, to be compared to a 5-year increase in the base case scenario. We account for death related costs by distinguishing the costs of survivors and decedents.10
This increase in life expectancy is calculated to imply a 0.4 percentage point increase in the ratio of acute health care expenditure to GDP, mainly because it expands the population that consumes health over a longer period of time. Expenditures on long-term care will increase on a similar scale. A decline in mortality rates will also increase pension expenditures as the number of people eligible for pension benefits will increase and will receive pensions for a longer time. The increase in life expectancy will lead to an additional increase of the ratio of public pension expenditure to GDP of 1.4 percentage points.
An increase in life expectancy of 3.2 years raises the sustainability gap with a 1.0 percentage point: in order to keep government finances sustainable, the primary surplus in terms of GDP needs to be increased by an additional 1.0 percentage points.
The ‘living in better health’ scenario
In this scenario we have investigated how a general improvement in health status will influence projections on age-related expenditures and public finances. Several studies11 have shown that disability rates among the elderly have declined and that the health status of the elderly has in general been improving. Assuming that the more recent trend of worsening health due to overweight and obesity will slow down, the historical trend of improving health may continue for the coming decades.
Continuous improvements in health have at least two effects. First, healthier people will need less medical attention. Second, an increase in health may postpone early retirement and reduce the inflow into disability schemes. This increases labor force participation and reduces expenditures on social security for people aged 55 and over.
In our calculations we assume that health status will improve according to the corresponding change in life expectancy in good health.12 This implies that in the period between 2000 and 2050 the remaining life expectancy in good health will increase with 8 years for cohorts with age 15 and 5 years for cohorts with age 65. Following Börsch-Supan (2000), we further assume that a 1% improvement in health status will lead to 0.8% fewer people quitting the labor force prematurely. Building on Lubitz et al. (2003), we also assume that among the group of those aged 65 and over, healthier persons will on average spend 20% less on health care than people with health problems. Furthermore, we assume, following a large empirical literature, that health care expenditure increases directly in line with GDP.
Our calculations show that an improvement in health will lead to a reduction in average expenditure on acute health care by 0.8% of GDP. An improvement in health status likewise leads to a lowering of expenditures on long-term care by 0.2% of GDP. The savings on long-term care expenditures are smaller than those on acute health care expenditure. Countries spend less on long-term care, so the savings on it are correspondingly less large. In addition, long-term care is consumed more heavily by older people, for which the relation between health status and expenditure can be considered to be weaker than for the 65- cohorts. An improvement in health will lead to a decline in the number of recipients of disability benefits in the age category of 55-64 years and thus expenditures. Total expenditures on public pensions will decline by 0.9%. The sustainability gap will decline with 0.8% of GDP compared with the base case scenario (see Table 1).

The ‘living longer in better health’ scenario
This scenario combines the two previous scenarios. ‘Living longer in better health’ will reduce expenditures on acute health care. The savings from health improvements thus dominate the effect that results from an increase in longevity. For long-term care expenditure the picture is opposite. Now the longevity effect dominates the health effect. For public pensions the ‘living longer’ effect also dominates the effect of better health.
The effect of living longer in better health on public expenditure can be seen to be relatively small: the sustainability gap increases with only a 0.1 percentage point. The drop in public spending due to healthier lives thus more or less neutralizes the boost in spending on account of longer lives.
Policy implications Official projection studies indicate that public finances are unsustainable in many countries in the world. EC (2009) calculates that government policies are unsustainable in most EU countries. The sustainability gap for the average EU country is calculated at 6.5 % of GDP.13 As indicated before, the size of the demographic changes ahead is difficult to predict. The same holds true for the variables that shape the macroeconomic environment, like for example, the world interest rate and the rate of GDP growth. This uncertainty surrounding future projections renders it difficult to assess precisely the size of the fiscal sustainability problem. Our calculations show that it is highly unlikely that there actually is no sustainability problem, however. In the ‘best’ of the scenarios considered, the sustainability gap could be 0.8% GDP smaller. This underscores the need for policy reform.
What would happen if policymakers for whatever reason were reluctant to take action? Clearly, public deficits and debts would increase. Such increases could continue for some time, but certainly not indefinitely. The higher the levels that deficits and debts would achieve, the greater the probability that interest rates would at some point in time start to increase, reflecting reduced confidence in a country’s creditworthiness. This would only add to the sustainability problem; ultimately, policy action would thus become unavoidable. Obviously, the burden of adjustment would then have to be borne by a smaller group of generations, born in a time period possibly very different from the time period in which the sustainability problems were created. Many people therefore consider this ‘wait and see’ policy option unfair.
A policy reform that would be implemented right now would both imply a smaller sustainability problem and a higher degree of generational balance, as the burden of adjustment would be spread over more generations. Such a policy option features also a drawback, however. In particular, part of the burden of adjustment falls upon the currently old generations, who did not anticipate policy reforms earlier in their lifecycles. Therefore, this policy option is often considered intergenerationally unfair as well.
A policy reform that could be said to lie in the middle of the two previous options is one in which it is decided now to take action in the not too distant future. This would relieve the burden imposed on the currently old generations and allow other generations to anticipate the reforms, while avoiding that the problems would increase to the same degree as in the ‘wait and see’ option. Many types of policy reforms can be considered. One example of such a reform would be to increase the future pension entitlement age, possibly on a step-by-step basis. One way to implement this would be to link the pension eligibility age automatically with life expectancy at birth, for example by including this link in law as is already done in several EU countries. Another one would be to reduce the scope of health insurance in the future, for example by a greater reliance upon co-payments or elements of private insurance.
The authors thank Winnie van Heesch and Marcel Lever for comments on a draft of this paper.
About the authors
Frank Pellikaan and Ed Westerhout Ed Westerhout is project leader at CPB Netherlands Bureau for Economic Policy Analysis of the Netspar theme Multi-pillar pension schemes and macroeconomic performance. He has been affiliated with the research department of the Ministry of Economic Affairs and the University of Amsterdam where he has been teaching economic growth, monetary and fiscal policies. At CPB, he has been leader of projects on ageing, pension reform and the health care sector. Ed Westerhout has published in leading academic journals such as International Tax and Public Finance, and Health Economics.
Notes 1.United Nations (2009). 2.Soares (2005). 3.United Nations (2009). 4.Murphy and Topel (2006). 5.The old age dependency ratio is defined as the ratio of elderly (65 and over) to the working age population (20-64). 6.Jacobzone et al. (2000), Cutler (2001). 7.Sturm et al. (2004). 8.Oeppen and Vaupel (2002). 9.Pellikaan and Westerhout (2005). 10.Pellikaan and Westerhout (2005). 11.Jacobzone et al. (2000), Cutler (2001). 12.Our research was part of the Ageing, Health and Retirement in Europe (AGIR) project (Mortensen (2005)). The data on life expectancy in good health that we have used in our study are also drawn from the AGIR project. 13.As this figure does not include the recent financial crisis, it very likely underestimates the current sustainability gap.
References
• Börsch Supan, Axel, 2000, Incentive Effects of Social Security on Labor Force Participation: Evidence in Germany and across Europe, Journal of Public Economics 78, pp. 25-49.
• Cutler, David (2001), Declining Disability among the Elderly, Health Affairs 20, pp. 11-27.
• European Commission (2009), Sustainability Report 2009, European Economy 9, Luxembourg.
• Jacobzone, S, E. Cambois and J.M. Robine (2000), Is the health of older persons in OECD countries improving fast enough to compensate for population ageing? OECD Economic Studies 30, pp. 149-190
• Lubitz, James, Liming Cai, Ellen Kramarow and Harold Lentzner (2003), Health, Life Expectancy, and Health Care • Spending among the Elderly, New England Journal of Medicine 349, pp. 1048-1055.
• Meier, Volker and Martin Werding (2010), Ageing and the Welfare State: Securing Sustainability, Oxford Review of Economic Policy 26, pp. 655-673.
• Mortensen, Jørgen (2005), Ageing, Health and Retirement in Europe, The AGIR Project, Final Report on Scientific Achievements, ENEPRI Research Report no. 11, July.
• Murphy, Kevin M. and Robert H. Topel (2006), The Value of Health and Longevity, Journal of Political Economy 114, pp. 871-904.
• Oeppen, Jim and James W. Vaupel (2002), Broken Limits to Life Expectancy, Science 296, pp. 1029-1031.
• Pellikaan, Frank and Ed Westerhout (2005), Alternative Scenarios for Health, Life Expectancy and Social Expenditure, ENEPRI Research Report no. 8, June.
• Soares, Rodrigo R. (2005), Mortality Reductions, Educational Attainment, and Fertility Choice, American Economic Review 95, pp. 580-601.
• Sturm, Roland, Jeanne S. Ringel, and Tatiana Andreyeva (2004), Increasing Obesity Rates and Disability Trends, Health Affairs 23, pp. 199-205.
• United Nations (2009), World Population Ageing, Department of Economic and Social Affairs, Population Division, New York.
• Vaupel, James W. (1998), Demographic Analysis of Aging and Longevity, American Economic Review 88, pp. 243-247.
White, K.M. (2002), Longevity Advances in High-Income Countries, 1955-96, Population and Development Review 28, pp. 59-76.



























































{kind=link}